









Severe pericardial effusion (PE) is a potentially severe clinical entity. Idiopathic PE accounts for one-third of patients with severe PE. However, evidence-based treatments are scarce. The aim of the study was to investigate whether pericardial drainage is associated with prognostic improvement, and to evaluate the influence of anti-inflammatory treatment on prognosis.
MethodsAll severe PE diagnosed between 2003 and 2017 were retrospectively collected. Of them, those classified as idiopathic were selected (N=153). Patients were divided in 2 groups: those who underwent pericardial drainage (N=105) and patients who did not (N=48). In addition, the study population was divided according to the anti-inflammatory drug (AD) administration. Median follow-up was 47.7 months.
ResultsThere were no significant differences in 2-year mortality between patients who underwent pericardial drainage and those who did not. There were also no significant differences in the number of hospitalizations for heart failure between the 2 study groups. However, mortality was significantly lower among patients who received AD compared to those who did not receive these agents. Only treatment with AD (HR, 0.24; P=.002) remained independently associated with lower mortality in the multivariate analysis. AD treatment was associated with a 70% reduction in mortality (HR, 0.30; 95%CI, 0.10–0.90; P<.031).
ConclusionsPericardial drainage was not associated with a better prognosis of patients with severe idiopathic PE, in terms of 2-year mortality, heart failure admissions, or the combined endpoint. AD treatment was found to be an independent protective factor for mortality in this patient population.
El derrame pericárdico (DP) grave es una entidad potencialmente grave. Hasta un tercio de los casos son catalogados de origen idiopático. Sin embargo, la evidencia acerca del tratamiento es escasa. El propósito de este estudio fue investigar si el drenaje pericárdico se asocia a una mejoría en la supervivencia global, y evaluar la influencia del tratamiento antiinflamatorio (TA) en el pronóstico.
MétodosSe recogieron retrospectivamente todos los casos de DP grave diagnosticados entre 2003 y 2017. De ellos, se seleccionaron los clasificados como idiopáticos (n=153). Los pacientes se dividieron en 2 grupos: aquellos que se drenaron (n=105) y los que no (n=48). Además, se subdividió a la población dependiendo del uso del TA. La mediana de seguimiento fue de 47,7 meses.
ResultadosNo existieron diferencias significativas en la mortalidad a 2 años entre los pacientes que recibieron drenaje pericárdico y los que no. Tampoco hubo diferencias entre el número de hospitalizaciones por insuficiencia cardiaca. Sin embargo, la mortalidad fue significativamente menor entre los que recibieron TA, en comparación con los que no. Solo el TA se mantuvo como un factor protector (HR: 0,24; p=0,002) en el análisis multivariado. El TA se asoció con una reducción de la mortalidad del 70% a 2 años (HR: 0,30; IC 95%; 0,10-0,90; p<0,031).
ConclusionesEl drenaje pericárdico no se asoció con una mejoría en el pronóstico en pacientes con DP grave de origen idiopático a 2 años, ni con una disminución en el número de ingresos por insuficiencia cardiaca o el objetivo combinado de ambos. El TA se mostró como un factor protector en esta población.
The best management of severe pericardial effusion (PE) in patients without clinical signs of cardiac tamponade remains controversial nowadays.1 Some authors recommend drainage in all cases of severe PE in order to restore pericardial anatomy and prevent future episodes of effusion.2 However, other authors propose drainage only in those situations in which there is clear evidence of cardiac tamponade, individualizing treatment in each patient.3,4 This last therapeutic approach could be justified considering the low diagnostic value of the biochemical analysis of pericardial fluid and the questionable value of pericardial biopsy.5,6
Idiopathic PE accounts for approximately one-third of patients with severe PE analyzed in multiple studies involving Western populations.7 Most of these cases have an uncertain cause and are often hypothetically related to possible viral infection and the subsequent inflammatory response to it.8 For this reason, the effusion can decrease and recurrence rates are reduced with the use of different anti-inflammatory drugs (AD).9,10
PE is a potentially severe clinical entity and even small PE has been related to an impaired prognosis.11 We aimed to elucidate whether an invasive approach with drainage is better than conservative management in patients with severe idiopathic PE. Furthermore, as a secondary endpoint, our aim was to study if AD make a difference in their prognosis.
MethodsAll consecutive patients who were admitted to a tertiary care centre with diagnosis of severe PE between 2003 and 2017 were retrospectively analyzed. The study was approved by the local Clinical Research Ethics Committee of Hospital Clínico San Carlos.
The severity of PE was assessed according to the recommendations of the European Society of Cardiology (ESC).1 To avoid potential sources of bias, all the echocardiographic images were analyzed in a Core Lab by an expert in cardiovascular imaging. The sum of the maximum PE diameter on the same echocardiographic subcostal plane was recorded. PE was defined as severe when this sum was greater than 20mm in diastole. Only patients with severe PE were considered for analysis. The echocardiographic assessment also included data on the location of the effusion, its distribution (circumferential or loculate) and a description of its appearance. Echocardiographic signs of haemodynamic compromise were considered as recommended in the guidelines.1,12,13 None of the patients included had clinical cardiac tamponade as well as haemodynamic instability.
When drainage of PE was performed, pericardial fluid samples were obtained and an aetiological study was performed, including biochemical analysis of the pericardial fluid, microbiology and cytology assessment, along with certain specific tests depending on the suspected diagnosis (such as Mantoux test or Zhiel-Nielsen stain in cases of suspected tuberculosis). In addition, all patients, either if drainage was performed or not, underwent a detailed anamnesis and physical examination. An electrocardiogram, blood test, and chest X-ray was obtained in all patients, as well as individual complementary tests. All cases were classified according to the primary aetiology (Fig. 1).

Inflammatory PE was diagnosed in those patients fulfilling more than 1 criteria of acute pericarditis, as recommended in ESC guidelines for the diagnosis and management of pericardial diseases1: (a) symptoms of acute pericarditis (pleuritic chest pain radiating to the shoulders, presenting in decubitus or with effort), (b) compatible electrocardiogram (newly discovered ST-segment elevation or decreased PR segment), (c) appearance of pericardial rubs and/or (d) PE (recently diagnosed or increased if previously present), along with elevation of acute phase reactants or evidence of inflammation in imaging tests such as computed tomography or cardiac magnetic resonance. Idiopathic PE was considered in those patients in which an aetiological diagnosis could not be achieved after a comprehensive study.
For the purposes of the present study, only patients with idiopathic PE were included in the analysis. All cases in which a definitive diagnosis, such as oncological or systemic disease, was made up to 2 years after the recruitment were excluded from the analysis. Clinical, analytical and echocardiographic variables were collected.
Patients were classified in 2 groups: those who underwent PE drainage (n=105) and those not drained (n=48). Drainage was performed in most patients by a standard subxiphoid pericardiocentesis, according to the Acute Cardiac Care Unit protocols of our centre. When subxiphoid access was not possible, the apical approach was used. The type of anti-inflammatory treatment and duration of the AD therapy were also recorded. Decision on when to perform pericardiocentesis and the AD selection was left to the treating physician in each case. At least 1 echocardiogram was performed after diagnosis of severe PE before discharge and in each clinical visit in all patients. After discharged, all patients were followed up in a dedicated clinic.
For purposes of analysis, only patients diagnosed with the first episode of idiopathic PE were included in the study (Fig. 1). The primary endpoint was 2-year overall survival between the 2 therapeutic strategies. We also aimed to assess differences in hospital re-admissions due to heart failure at 2 years between the 2 study groups; and the combined endpoint of mortality or hospital admissions due to heart failure. Another objective of our study was to evaluate differences in prognosis and mortality between those patients who received/not received AD for the treatment of severe PE.
Baseline characteristics and clinical events between groups were compared in the univariate analysis. A multivariate Cox regression analysis was performed to evaluate potential prognostic markers. We included in the model those variables that resulted statistically significant in the univariate analysis as well as other clinical and echocardiographic variables previously known to be associated with prognosis or those clinically relevant for the analysis of the primary endpoint.
Continuous variables are reported as mean±standard deviation in case of a normal distribution or median and interquartile range in case of asymmetry. Groups were compared by the unpaired Student t test, or Mann–Whitney U and Kruskal–Wallis tests in cases of significant deviation from the normality assumption (P<.05 in the Kolmogorov–Smirnov or Shapiro–Wilks tests). Categorical variables are reported as counts and proportions and compared with the chi-square test or Fisher's exact test when the expected count in any cell of the 2×2 table was <5. Variables with a P value<.10 in univariate analyses were considered for the multivariate models. Multivariate Cox proportional risk analyses were made by a stepwise backward elimination technique, and only variables with a P value<.05 were used in the final model. Kaplan–Meier survival analysis was used to compare primary and secondary endpoints and differences were assessed with the log rank test. Statistical significance was set at 0.05. Statistical analysis was performed with Stata 14 package, StataCorp LLC.
ResultsDuring the study period, 461 patients were diagnosed of severe PE, 153 (33.3%) of them were finally classified as idiopathic and they form our study sample (Fig. 1). Baseline characteristics and differences between patients who were drained and those were not are shown in Table 1. Those patients who underwent pericardial drainage had larger PE and echocardiographic signs of haemodynamic compromise were more common in this group. There were no significant differences in other relevant characteristics such as age, serum creatinine level or Charlson comorbidity index (Table 1). In order to assess factors associated with the presence of echocardiographic signs of haemodynamic compromise, we performed a multivariate logistic regression analysis. Only the size of the effusion was independently associated with the presence of echocardiographic signs of compromise (Table 1 of the supplementary data).
Baseline characteristics of 153 patients with severe pericardial effusion of idiopathic origin.
| Characteristics | Drained (n=105) | Not drained (n=48) | P |
|---|---|---|---|
| Age (years) | 70.4±15.4 | 73.5±18.5 | .279 |
| Male sex | 62 (59.1) | 27 (50.0) | .295 |
| Smoking habit | .496 | ||
| Current smoker | 65 | 34 | |
| Past smoker | 28 | 9 | |
| Non smoker | 12 | 5 | |
| Anticoagulation | 21 (20.0) | 8 (16.7) | .238 |
| Fever | 27 (25.7) | 12 (25.0) | .925 |
| Previous myocardial infarction | 1 (1.0) | 1 (2.1) | .567 |
| Signs of haemodynamic compromise | 51 (48.6) | 7 (14.6) | .001 |
| Maximum diameter (mm) | 35.7±12.0 | 30.3±9.1 | .007 |
| Treatment with antiinflammatory drugs | 43 (41.0) | 16 (33.3) | .369 |
| Creatinin (mg/dL) | 1.3±0.8 | 1.2±0.6 | .422 |
| Charlson comorbidity index | 4.8±2.7 | 4.8±2.5 | .873 |
| C-reactive protein (mg/L) | 7.9±1.4 | 7.5±0.9 | .797 |
Data are expressed as no. (%).
Median follow-up was 47.7 months [IQR 14.2–91.3 months]. Fifty-nine (38.6%) patients were treated with AD. Of them, 23 were treated with nonsteroidal AD (15.0%), 6 with colchicine in monotherapy (3.9%), 9 with corticosteroids (5.9%), 18 with a combination of nonsteroidal AD and colchicine (11.8%) and 3 with other combinations (2.0%). Median duration of the AD therapy was 6 weeks [IQR 4–12 weeks].
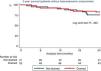
During the 2-year follow-up, 33 (21.6%) patients died. There were no significant differences in 2-year global mortality between patients who underwent pericardial drainage and those who did not (OR, 0.90; 95%CI, 0.44–1.87; P=.784 (Fig. 2A). After stratifying by AD treatment, differences in 2-year mortality between patients who underwent drainage and those who did not, remained non-significant (OR, 1.13; 95%CI, 0.12–10.88; P=.915 in patients treated with AD and OR, 1.01; 95%CI, 0.46–2.18; P=.990 in patients not treated with AD). However, mortality was significantly lower among patients who received AD therapy compared to those who did not receive these agents (Fig. 2B). After excluding those patients with echocardiographic signs of haemodynamic compromise, AD remained associated with better prognosis in the stratified analysis, independently of pericardial drainage (Fig. 1 of the supplementary data). There were also no significant differences in the number of hospitalizations for heart failure (OR, 4.11; 95%CI, 0.52–32.44; P=.180) and the combined endpoint (mortality or hospitalizations for heart failure) between patients who were drained and those who did not (OR, 1.20; 95%CI, 0.58–2.46; P=.629) (Fig. 3). In order to assess the potential impact of the presence of echocardiographic signs of haemodynamic compromise on the results, survival analyses were stratified by this variable. Focusing on patients without echocardiographic signs of haemodynamic compromise, the survival analysis showed no differences in 2-year mortality between those patients who underwent PE drainage and those who did not independently of the presence of echocardiographic signs of compromise (Fig. 4). Results of univariate and multivariate analysis to predict mortality are shown in Table 2. Treatment with AD was independently associated with lower mortality in the multivariate analysis (Table 2). In addition, age was significantly associated with higher mortality and creatinin levels showed a non-significant association with mortality, after multivariate adjustment. Drainage of PE resulted statistically non-significant in the multivariate analysis for prediction of mortality.

(A) Kaplan–Meier survival analysis in 153 patients with severe idiopathic PE between patients who were drained (red line) and those who were not (blue line). (B) Kaplan Meier survival analysis in 153 patients with idiopathic severe pericardial effusion stratified by anti-inflammatory drugs (AD) treatment. Four therapeutic alternatives are represented: drainage and AD treatment (solid red line), drainage and no AD treatment (dashed red line), no drainage and AD treatment (solid blue line) and no drainage/no AD treatment (dashed blue line). This figure is shown in full colour only in the online version of the article.


Univariate and multivariate analysis to predict 2-year mortality.
| Mortality | ||||||
|---|---|---|---|---|---|---|
| Univariate | Multivariate | |||||
| HR | 95%CI | P | HR | 95%CI | P | |
| Age (by 1 year increment) | 1.07 | 1.04–1.11 | .001 | 1.06 | 1.02–1.10 | .004 |
| Male sex | 0.88 | 0.44–1.76 | .711 | |||
| Smoking habit | 4.30 | 0.59–31.47 | .151 | |||
| Anticoagulation | 1.27 | 0.55–2.94 | .574 | |||
| Fever | 1.16 | 0.54–2.51 | .706 | |||
| Maximum diameter (by 10mm increment) | 1.01 | 0.98–1.04 | .702 | |||
| Signs of haemodynamic compromise | 1.08 | 0.53–2.23 | .830 | |||
| Treatment with antiinflammatory drugs | 0.19 | 0.07–0.54 | .002 | 0.29 | 0.10–0.86 | .025 |
| Drainage | 0.90 | 0.44–1.87 | .784 | 1.42 | 0.68–3.00 | .354 |
| Creatinin (by 1mg/dl increment) | 1.46 | 1.04–2.05 | .030 | 1.51 | 0.99–2.30 | .054 |
| Charlson score index (by 1 point increment) | 1.37 | 1.20–1.56 | .001 | |||
Considering the main secondary objective, differences in baseline characteristics between patients who received AD treatment and those who did not are shown in Table 1 of the supplementary data. Patients who did not receive AD were older and had a higher Charlson comorbidity index (Table 3). This group of patients received more frequently anticoagulation due to other causes. On the other hand, fever was more common and levels of C-reactive protein higher among patients who received AD (Table 3). Despite that, AD administration remained independently associated with mortality reduction after multivariate adjustment.
Baseline characteristics of 153 patients with severe pericardial effusion of idiopathic origin. Differences between patients who received/did not received anti-inflammatory drugs.
| Characteristics | Treated with antiinflammatories (n=59) | Not treated with antiinflammatories (n=94) | P |
|---|---|---|---|
| Age (years) | 63.1±2.3 | 76.5±1.3 | .001 |
| Male sex | 31 (52.5) | 55 (61.4) | .469 |
| Smoking habit | .438 | ||
| Current smoker | 34 (57.6) | 65 (69.2) | |
| Past smoker | 15 (25.4) | 22 (23.4) | |
| Non smoker | 10 (17.0) | 7 (7.5) | |
| Anticoagulation | 24 (40.7) | 5 (5.3) | .009 |
| Previous cardiac surgery | 1 (1.7) | 0 (0.0) | .205 |
| Fever | 23 (39.0) | 16 (17.0) | .002 |
| Previous myocardial infarction | 1 (1.7) | 1 (1.1) | .738 |
| Signs of haemodynamic compromise | 19 (32.2) | 39 (41.5) | .229 |
| Maximum diameter (mm) | 33.4±1.4 | 33.3±1.1 | .639 |
| Creatinin (mg/dL) | 1.1±0.1 | 1.3±0.1 | .137 |
| Charlson Comorbidity Index | 3.5±0.3 | 5.6±0.2 | .001 |
| C-reactive protein (mg/L) | 9.7±1.2 | 5.8±0.9 | .008 |
Data are expressed as no. (%).
Severe PE is a relatively frequent entity, accounting for approximately 4% of all patients admitted to the emergency department with dyspnoea.14 Multiple studies have investigated different therapeutic approaches, especially for patients with PE of oncological origin, with good results over mortality rates both in patients who suffer cardiac tamponade and those who do not.15,16 However, although idiopathic effusion is one of the most frequent causes of severe PE, evidence based therapeutic options are scarce.1 The present study has several strengths that deserve consideration: to the best of our knowledge, this study is the largest one carried out with patients with severe PE of idiopathic origin, with a very long-term follow-up (median 47.7 months). In a recent study, Imazio et al. reported that patients with chronic idiopathic PE treated conservatively had a better prognosis than those who required intervention.17 Our results showed absence of significant differences in prognosis between patients who underwent pericardial drainage and those who did not. One key point of our study is the analysis of the potential value of the anti-inflammatory treatment in this patient population. In fact, we found that prognosis of patients treated with AD was much better than that of patients who did not receive this therapy. After 24 months of follow-up, survival of patients treated with AD was higher than 90% (93.2%), while less than 70% (69.9%) of patients not treated with AD remained alive at the end of the follow-up (Figs. 2B and 3). C-reactive protein levels were increased either in patients who received AD and those who did not. Interestingly, C-reactive protein levels were higher in patients who received AD. It is possible that intensity of inflammatory response may play a key role in some patients classified as idiopathic. Therefore, efforts should be may to identify those patients who may benefit from AD treatment. In this sense, C-reactive protein could be useful, as well as other inflammatory biomarkers.
Mortality rate of patients with severe PE has been reported to be 35–50% in different series.2,15 Our results showed a mortality rate just over 20% at 2 years, which is lower than that reported in previous studies.2,15 However, previous studies included heterogeneous patient populations with a great variety of PE aetiologies. A high proportion of patients included in previous studies were oncological. It is well known that these patients usually have a worse prognosis and higher mortality rates that those with a different aetiology of the severe PE.15,16 In our study, oncological patients and other specific aetiologies were excluded, and only patients finally classified as idiopathic PE were analyzed. Mortality rates and prognosis of patients with idiopathic PE is known to be better than that of oncological PE.
Our results show that routine drainage of patients with severe PE did not have an impact on mortality rates of patients with idiopathic PE. Although pericardiocentesis is a safe technique, and it is sometimes a necessary step in diagnosis of patients with severe PE, its value as a therapeutic option seems to be uncertain. In patients with echocardiographic signs of haemodynamic compromise, routine drainage is the most common approach and differences between drainage and conservative treatment are sometimes difficult to assess. However, in our series, 7 patients with haemodynamic compromise were medically managed with AD. Among them, 2-year mortality was similar to that of patients who underwent pericardial drainage in the same clinical situation. Moreover, among patients without echocardiographic signs of haemodynamic compromise, PE drainage did not make any difference in prognosis and mortality.
On the other hand, our results show that AD treatment was associated with a significant reduction in mortality (HR, 0.19, 95%CI, 0.07–0.54; P=.002) and this protective effect remained statistically significant after multivariate adjustment (HR, 0.30, 95%CI, 0.10–0.90; P<.031) (Table 2). The association of AD treatment with a better prognosis and reduction in mortality was independent of whether patients underwent PE drainage or not (Fig. 1). However, considering the limited number of patients included and the observational nature of the study, this effect should be tested in larger randomized studies.
Although in our study patients treated with AD were considerably younger and with a lesser number of comorbidities, AD treatment remained significantly associated with lower mortality after multivariate analysis. AD has been previously associated with a considerable reduction in recurrence of the PE when added to pericardial drainage,18 but also this study supports that it might have an impact on long-term prognosis. Several authors support the idea that AD should be part of the standard therapy in patients with inflammatory PE, independently of the drainage requirement.19 Furthermore, drainage of severe idiopathic PE should only be considered as a complementary approach to AD treatment in those patients with cardiac tamponade or as a diagnostic tool. Nevertheless, larger randomized studies are needed to prove these hypotheses.
LimitationsOur study has several limitations that should be considered when interpreting the results. This is a single-centre observational retrospective analysis, with limitations inherent of these types of studies. Specific causes of mortality were not known in 50% of the cases, although unknown cases were equally distributed in the 2 different treatment groups. Causes of death have been detailed in those patents in which this information was available (Table 2 and 3 of the supplementary data).
Although the median follow-up was 47.7 months [IQR 14.2–91.3 months], only data on 2-year follow-up were used in the multivariable and survival analysis, in order to avoid potential sources of bias. PE management, including pericardial drainage and the use of AD was not standardized, but decided by the treating physician and individualized in each case. Therefore, we cannot completely exclude that several factors such as renal impairment, age, comorbidities could have influenced this decision. However, AD treatment was independently associated with better prognosis in the multivariate analysis.
Besides that, although treatment with AD was associated with a reduction in mortality, there was a wide variety of AD treatment regimens in our study. Therefore, specific recommendation on the AD regimen cannot be made. Finally, there was a limited number of events during the follow-up. Therefore, the multivariate analysis may be insufficiently adjusted, as it is based on a short number of events.
ConclusionsIn patients with severe idiopathic PE, pericardial drainage did not influence 2-year all-cause mortality, heart failure re-admissions, or the combination of both. Treatment with AD was found to be an independent protective factor for mortality in this patient population. This protective effect was independent of whether patients underwent pericardial drainage or not.
- -
PE is a frequent cause of dyspnoea. Idiopathic PE accounts for approximately one-third of patients with severe PE.
- -
PE is a potentially severe clinical entity and even small effusions have been related to an impaired prognosis.
- -
The best management of severe PE in patients without clinical signs of cardiac tamponade remains controversial nowadays.
- -
AD may reduce recurrences in patients with acute pericarditis and significant PE.
- -
In patients with severe idiopathic PE, pericardial drainage might not improve prognosis, compared to medical treatment.
- -
Patients with greater PE and echocardiographic signs of haemodynamic compromise underwent drainage in a higher proportion.
- -
Treatment with AD was found to be an independent protective factor for mortality in this patient population with idiopathic PE.
There is no funding source to declare related to this study.
Conflicts of interestAll the authors state that there are no potential conflicts of interest related to this work.
The following are the supplementary data to this article:

Abbreviations: AD: anti-inflammatory drugs; PE: pericardial effusion.



