



Información del artículo
Texto completo
Bibliografía
Descargar PDF
Estadísticas
Tablas (2)
Table 1. Characteristics of the patients, signs, symptoms and outcome.
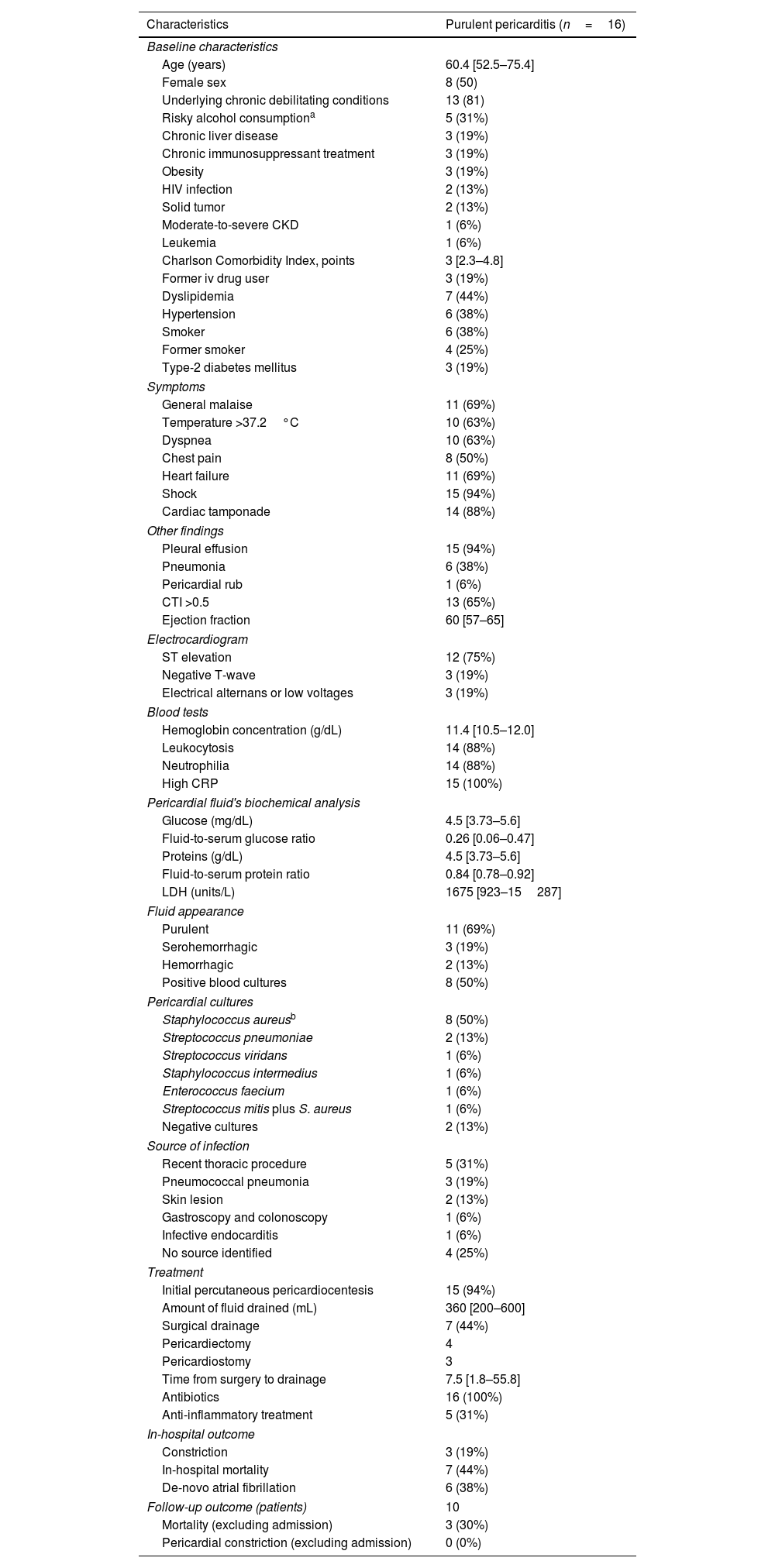
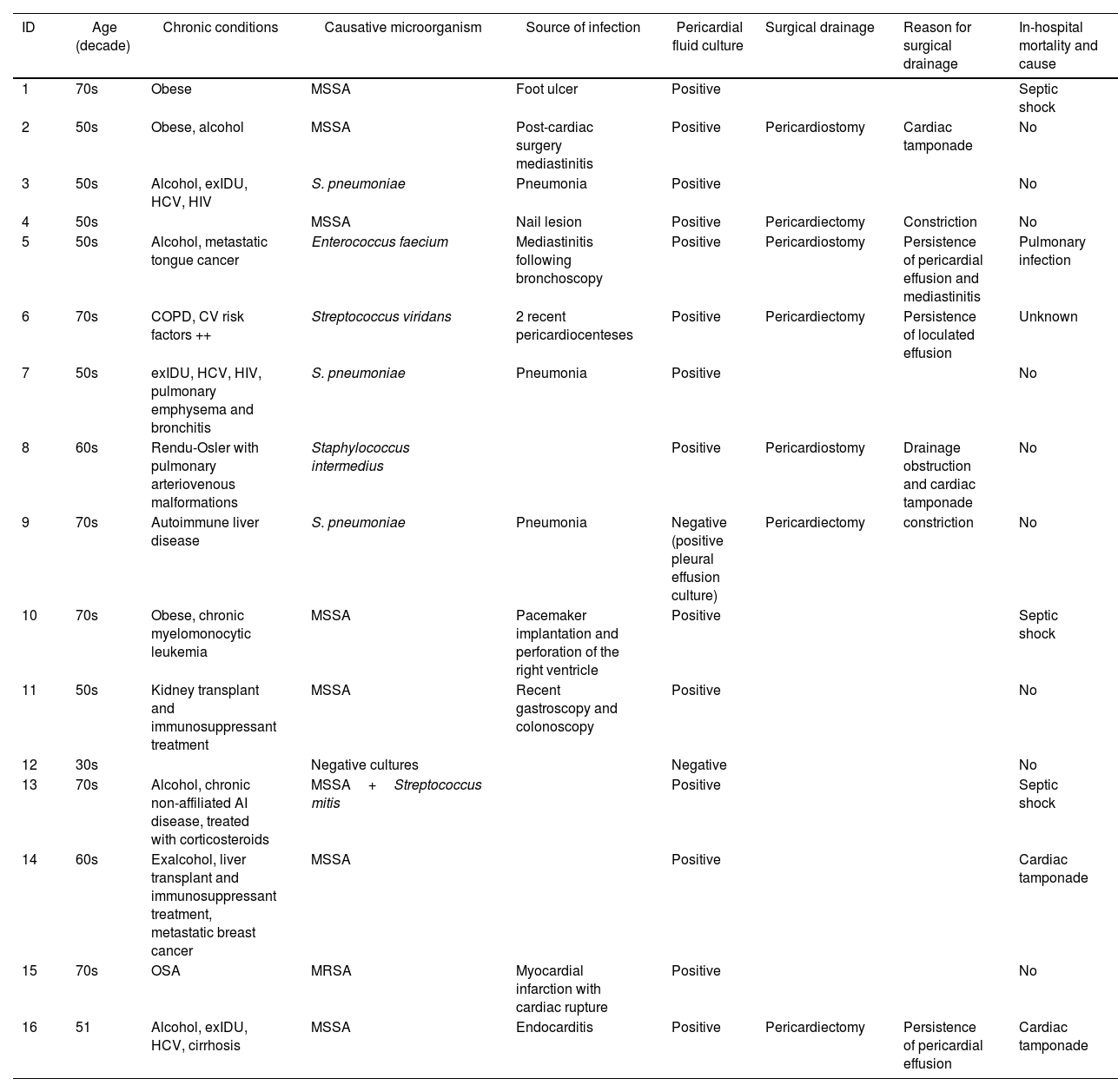
Table 2. Risk factors, causative microorganism, source of infection, treatment and in-hospital outcome of 16 adult patients with purulent pericarditis.
Mostrar másMostrar menos
Artículo
Opciones para acceder a los textos completos de la publicación
REC: CardioClinics
REC: CardioClinics
Socio
Socios SEC
Use datos de acceso a SEC en el menú Acceder.
Si es socio de la Sociedad Española de Cardiología y no puede acceder con sus claves, escriba a rec@cardioclinics.org.
Use datos de acceso a SEC en el menú Acceder.
Si es socio de la Sociedad Española de Cardiología y no puede acceder con sus claves, escriba a rec@cardioclinics.org.
Members of SEC
Use the Society's website login and password here.
If you are member of SEC and you have some problems with your login data, please contact with rec@cardioclinics.org.
Use the Society's website login and password here.
If you are member of SEC and you have some problems with your login data, please contact with rec@cardioclinics.org.
Suscriptor
Suscriptor de la revista
Si ya tiene sus datos de acceso, clique aquí.
Si olvidó su clave de acceso puede recuperarla seleccionando la opción "He olvidado mi contraseña".
Comprar
Comprar acceso al artículo
Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora
Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora



